(For readers new to Roam, the presence of double square brackets enclosing a word or a phrase indicates a link to a page that has that word or phrase as its title.)
Introduction
One of the things I do with my life is work as a pharmacist, although most of my interests have been in founding companies in transdermal drug delivery and the biology of ageing, particularly in skin. I’ve been using Roam since mid-December 2019, to try to pull together and make sense of scientific papers in biology and hopefully develop some insights. Covid-19 has put my company’s human and biochemical trials on hold for an extended period, and so I decided it was finally time to improve my clinical knowledge.
I’ve never liked clinical knowledge. It has never seemed “real” to me. Whereas pharmacology attempts to understand how drugs work at a molecular or system level, clinical knowledge is more about how you use something.
It’s like the difference between coding and using a word processor. You don’t need to know how the program is written to use “copy and paste”.
Clinical knowledge always felt to me like an untidy collection of “If.. (this set of circumstances).. then.. that, and if that doesn’t work then use this other thing, if other thing doesn’t work then (an authority) says add New Thing to other thing”. If none of that works, send the patient on to (specified someone else).
All very important, but not exactly intellectually satisfying. Heuristics, rules of thumb, flowcharts, recipes, trial and error, local guidelines, updated advice. My brain seemed to reject learning a million different “if..then..” scenarios.
Unhelpfully, the way clinical knowledge is presented is really not my “cup of tea”. I find it over-wordy: slabs of text with muddled but well-meaning infographics and flowcharts and a load of things the author thinks you “ought to know” or want to show you they know, even though they will not be useful.
You have to work hard to extract sense from it. And, even if you can extract actionable information, will you have that sheet of paper or email to hand when you need it? How much of that funky flowchart will you be able to remember? Will you be able to apply something in one context to another context, or will it be forever siloed? The whole process seems doomed to failure.
Recently, I was asked a question about use of ACE inhibitors in mild renal dysfunction, which I fortunately (or luckily) I got right. But I realised that I really ought to be learning more, and resolved to use my two passions, note-taking on Roam and spaced repetition memory development on Anki, to sort it out.
This blog post examines what I have been learning through the Roam element of this process.
The public Roam database I have created for clinical knowledge can be found here: roamresearch.com/#/app/ClinicalKnowledgeSummaries/page/_GaamAGYO.
Why might Roam be useful?
Working with Roam on clinical knowledge is not yet a common use scenario, but I have found that using Roam helps you to learn and interrogate many sorts of information in a really useful way.
The first benefit is that putting the information into Roam gives you control over it.
The way information is usually presented is like being handed a massive steak from the grill and a large baked potato straight from the oven. The first thing you need to do is put those things on a plate, otherwise they’re going to burn you within a couple of seconds and you’ll have to drop them. The next thing you’ll need to do is use some good quality cutlery to cut them up into smaller pieces to put them in your mouth one by one. Then you’re going to need to chew each piece, to get the food into a format and size that your stomach can handle. Then your body will break it down on a molecular level and assimilate the food, getting it ready to be used.
Roam first provides the plate to put the food on, then the nested levels provide the knives to chop it up into small enough pieces. Creating questions for spaced repetition helps to digest the information. Bidirectional links are the assimilation into the body of knowledge as a whole.
That’s the first part of Roam. I’ve never found a better method for digesting and assimilating information.
The next part is equally important – the ability to interrogate that information to provide actionable information quickly enough to be useful. Preferably, as quickly as the speed of human memory.
I want to get to a point where my Roam “knows” things, so that, in effect, it is irrelevant if that knowledge is stored in silicon media or my brain.
Choice of information base and method
I decided I needed a relatively homogenous and up-to-date base information source that I could base my Roam on. I chose the NICE (UK National Institute for Health and Care Excellence) Clinical Knowledge Summaries.
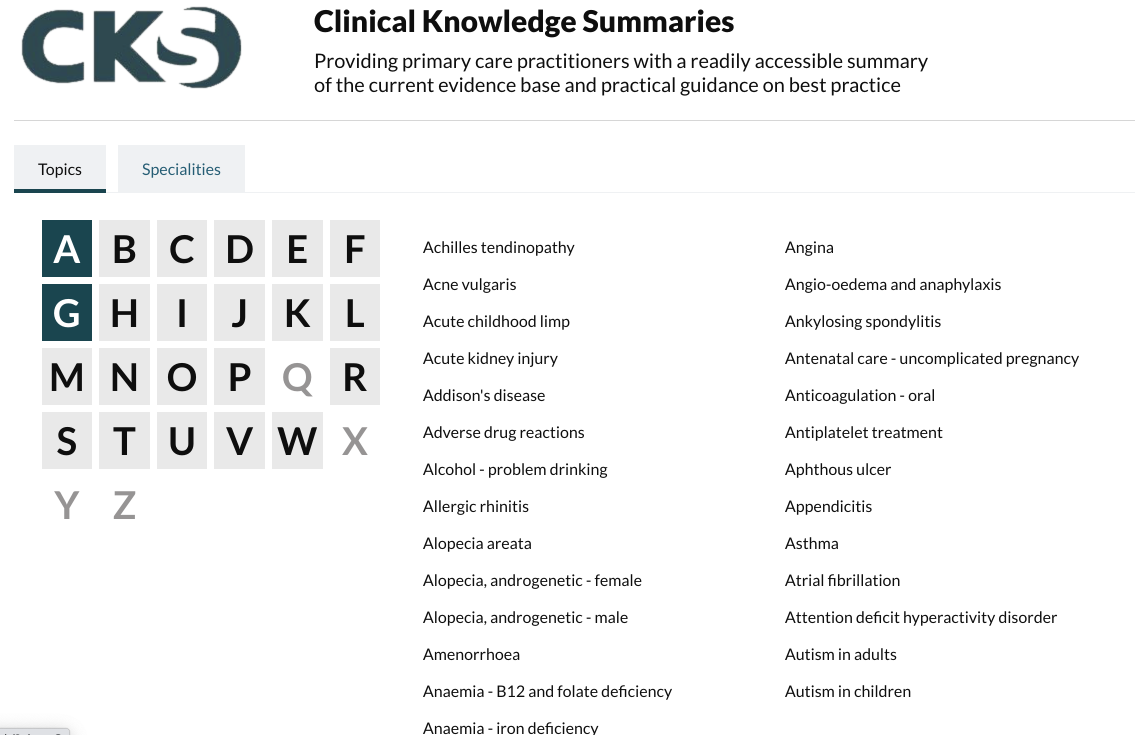
It had to be homogenous in structure, terminology and relatively internally consistent. So far it has turned out to be so. I’m working through from the most common problems seen in primary care (for example [[cardiovascular disease]] and [[diabetes]]) and then working out to the less common.
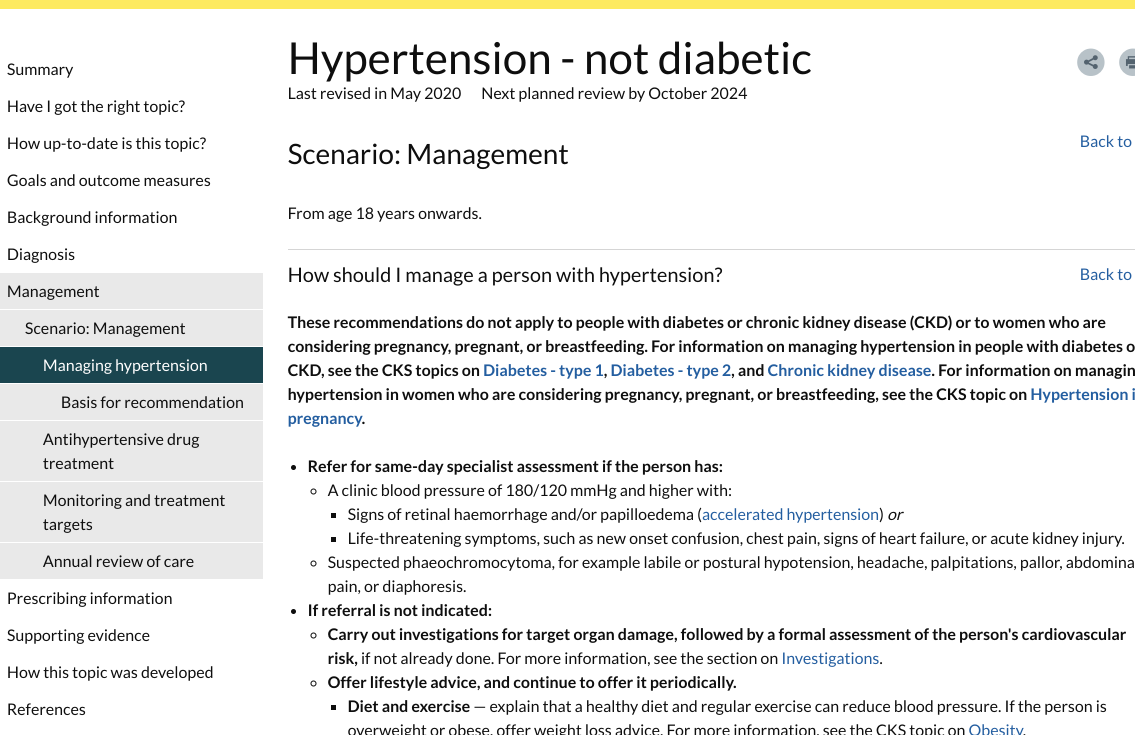
Here’s an example of a page on [[hypertension]]. Clearly it provides a good possibility to be converted to nested levels. The actual page scrolls down a really long way. This makes it difficult to find information, and hard to ascertain structure at a glance
Here’s my Roam version.
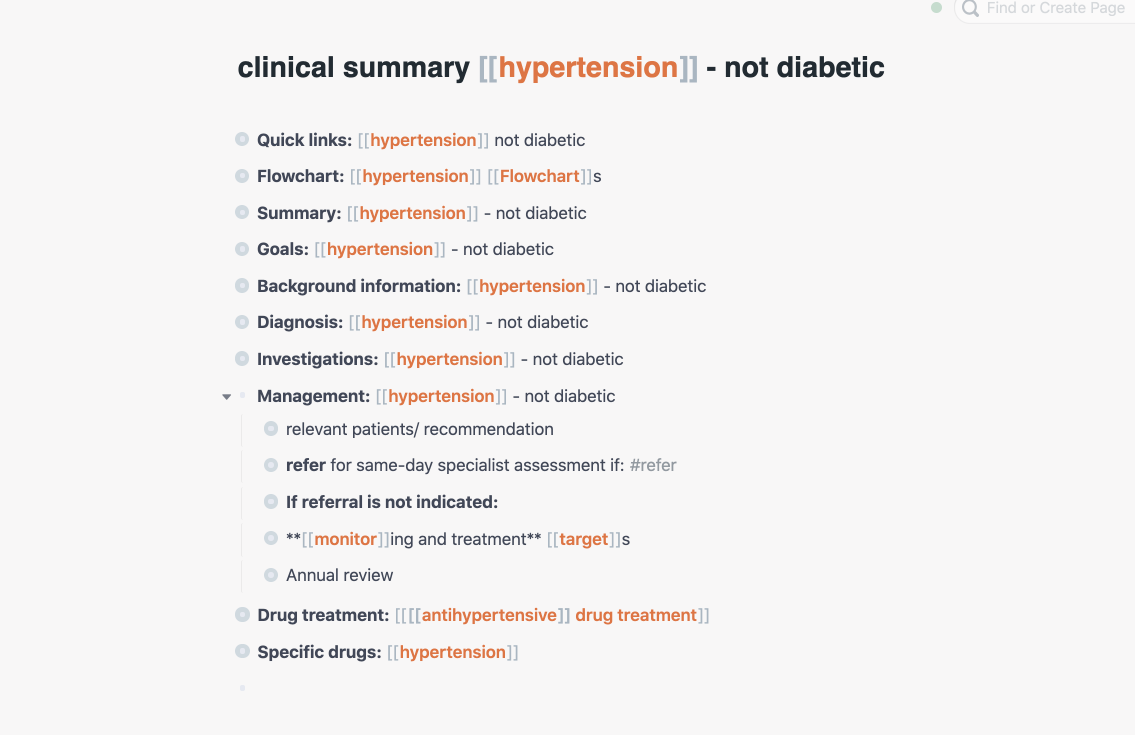
Then, as I drill down, each move preserves the structure of the information, and also shows the higher level context.
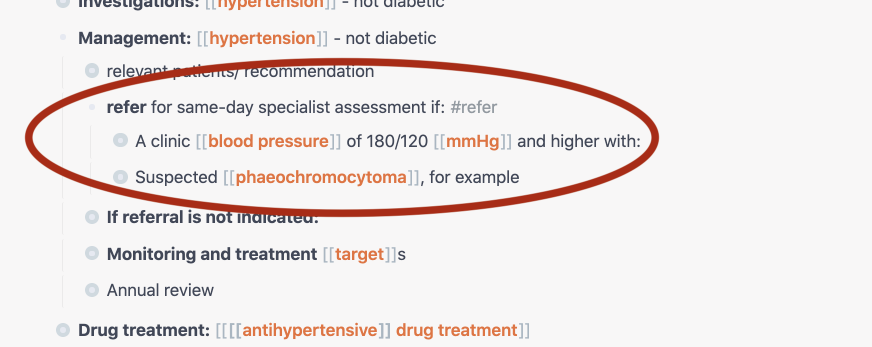
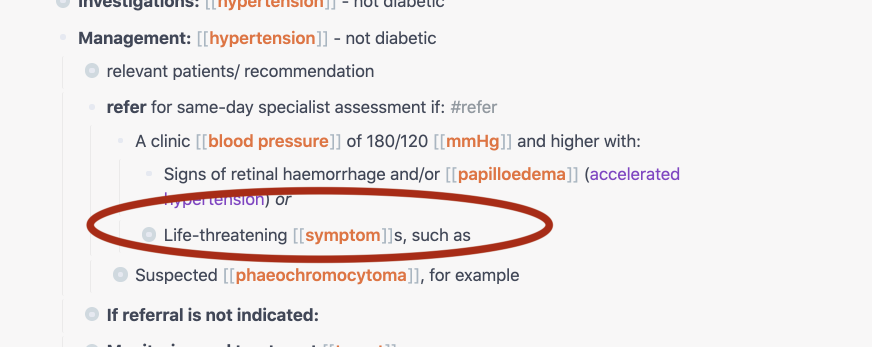
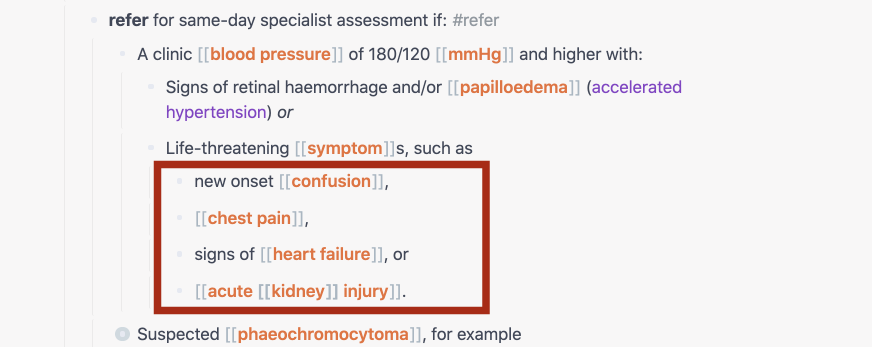
As you go through the levels, you only see what you need to see at each point, so you are not overwhelmed with text.
So far, so normal. This still feels a pretty traditional way of accessing information.
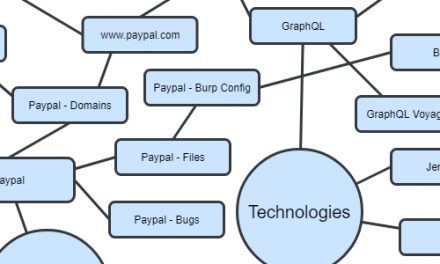
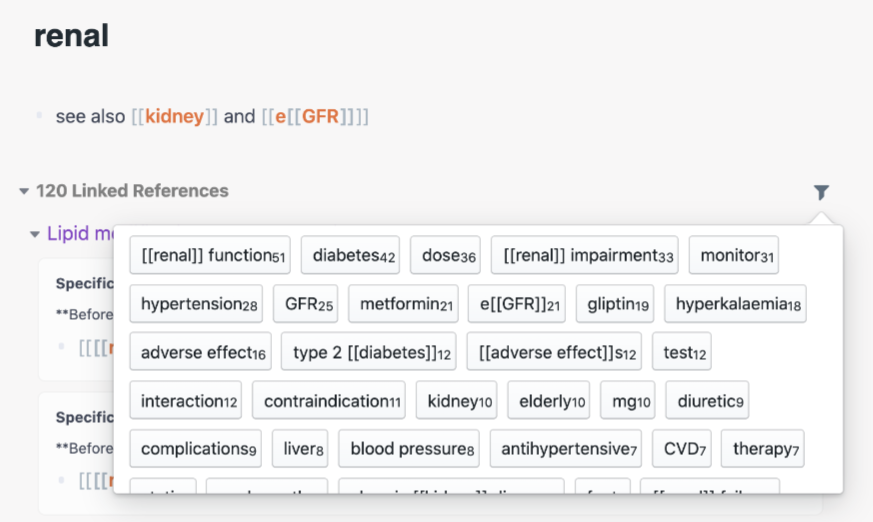
However what Roam also enables is to read across subjects and see where topics are joined up. For instance, from this information, I might want to see how renal problems might affect the management of a patient with a variety of conditions or drugs.

Looking for renal gives me a quick overview. If I press the filter button, I get an overview of associated words and topics.

But maybe that’s not specific enough.. Maybe I need to see how what information there is for this group of drugs in relationship to older people. I might add the filter “older”, and then get only three database hits.
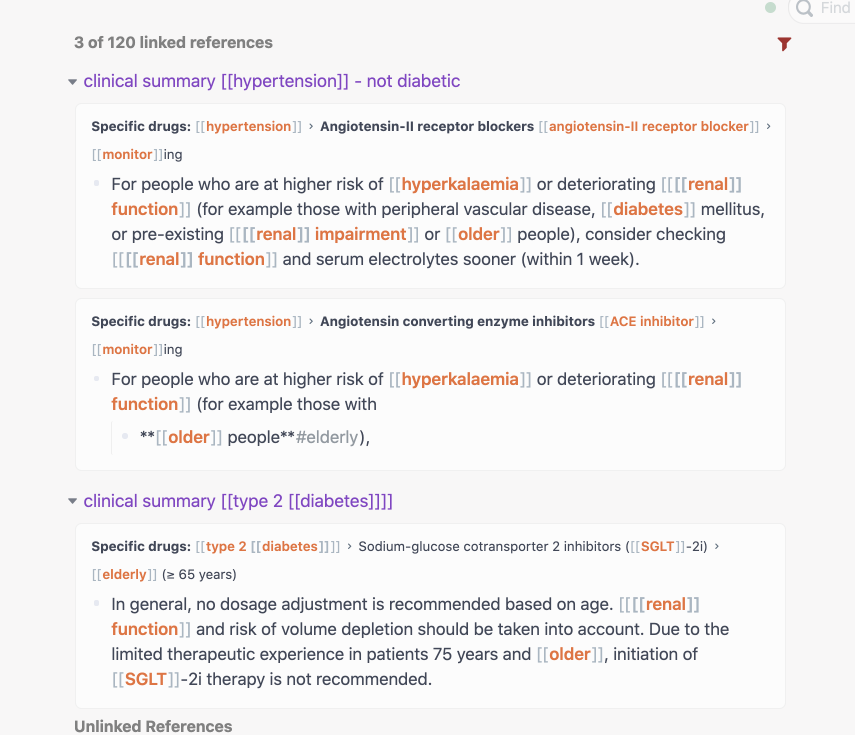
Using these filters, I can quickly get to the information I want whilst, at the same time, soaking up information about context, structure and other possibilities. What is helpful is that the most commonly associated concepts and words are at the top of the filter list.
Or I might want to look for [[contraindication]]s for a particular drug or group of drugs, such as thiazides.
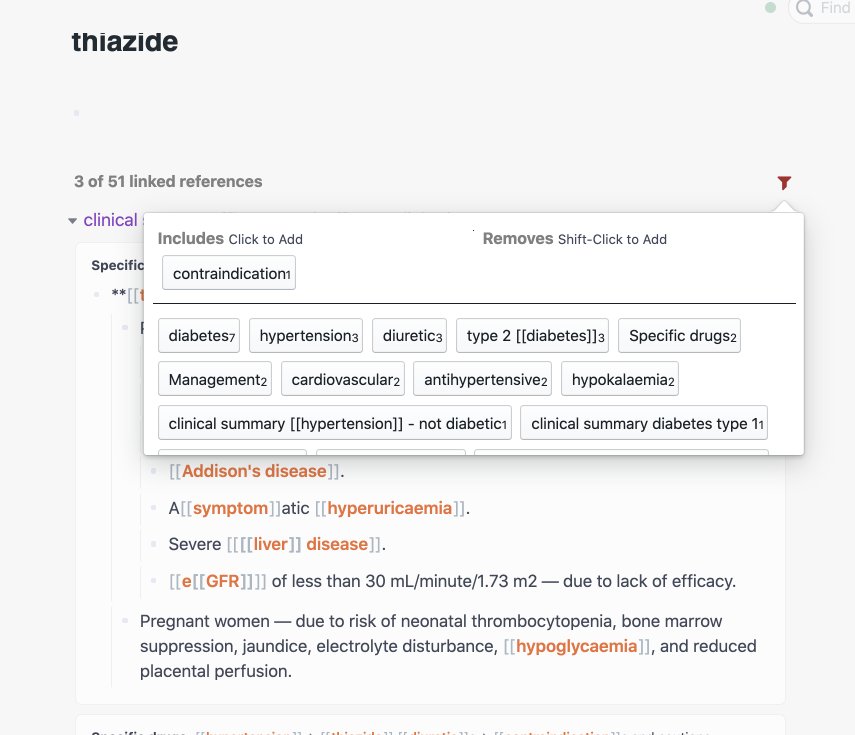
You get the picture. Roam also works really well in mobile, except I haven’t yet figured out how to shift-click to put a topic in the “remove” section for filtering.
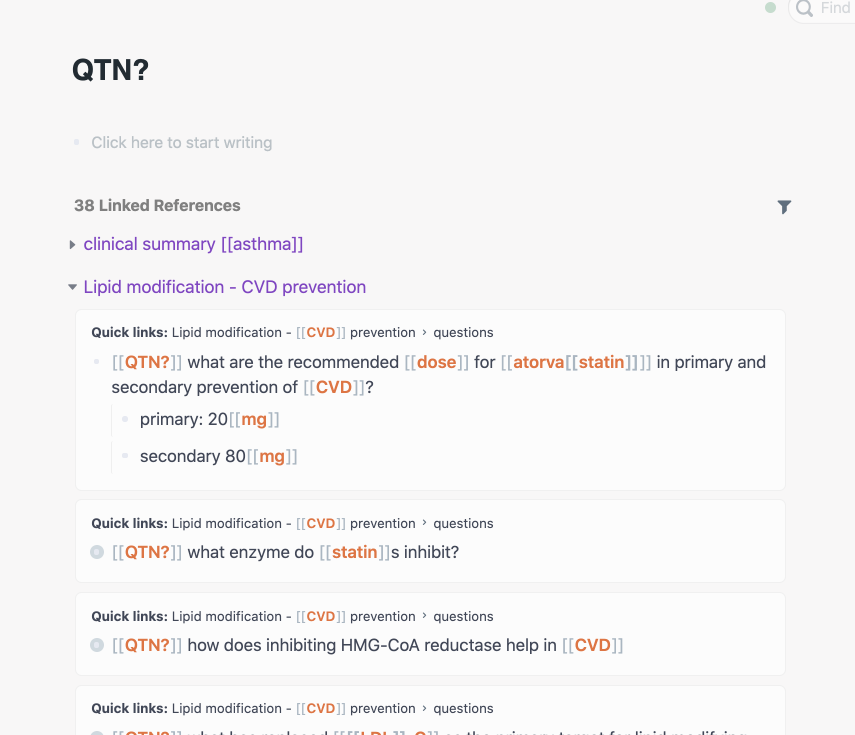
Here are some examples of questions that I have taken from Roam into Anki to help me remember some key concepts and information.
Converting flowcharts for Roam
Here’s an example of a flowchart on [[hypertension]].
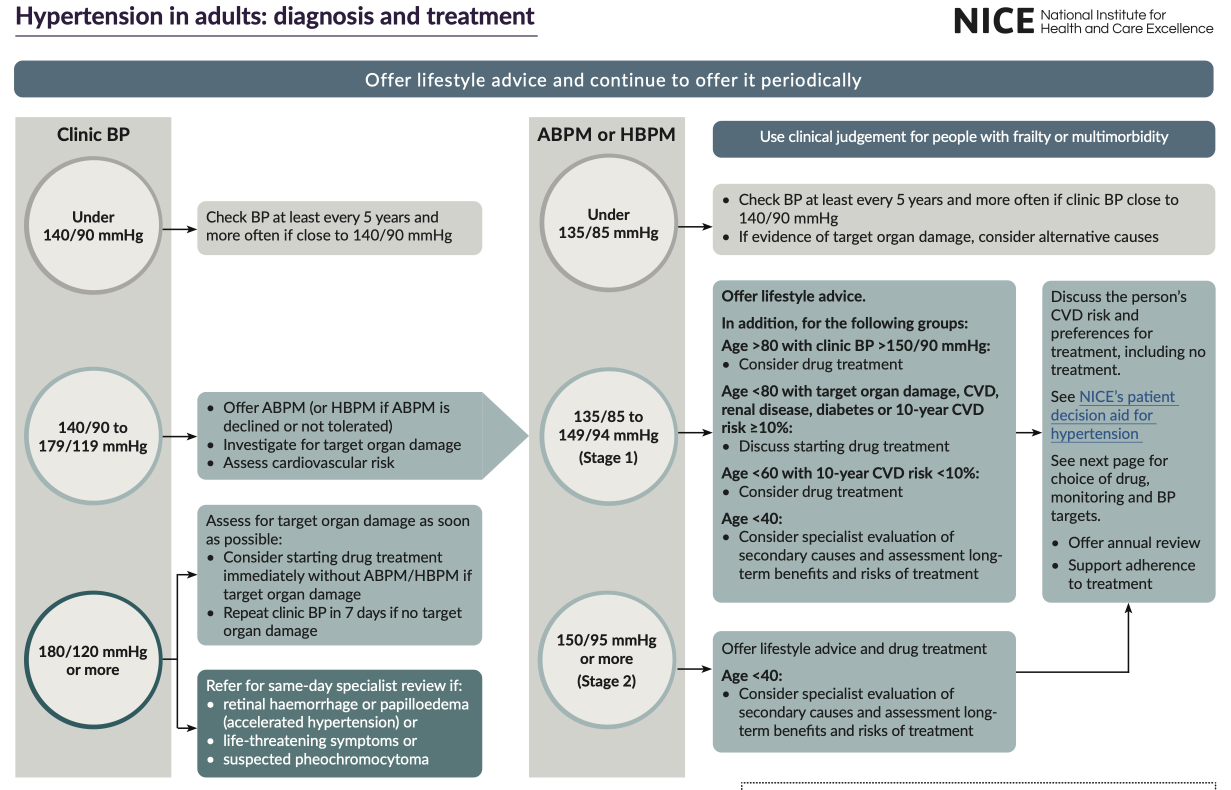
Although this information seems helpful, I find the format overwhelming. So I decided to see if flowcharts could be reformatted as nested levels.
This is what I came up with.
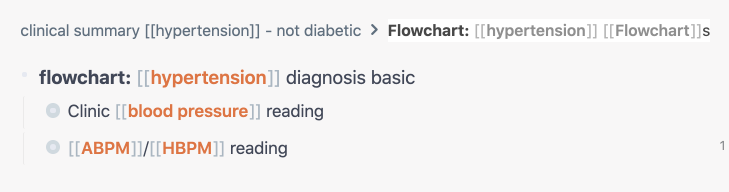
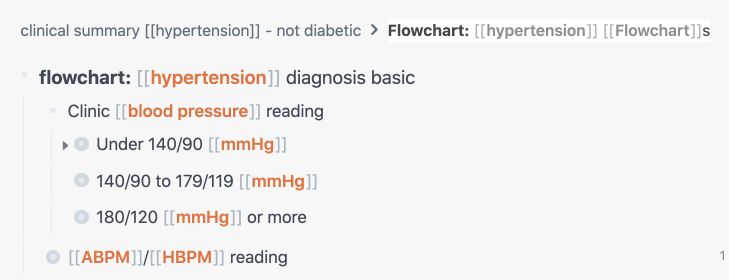
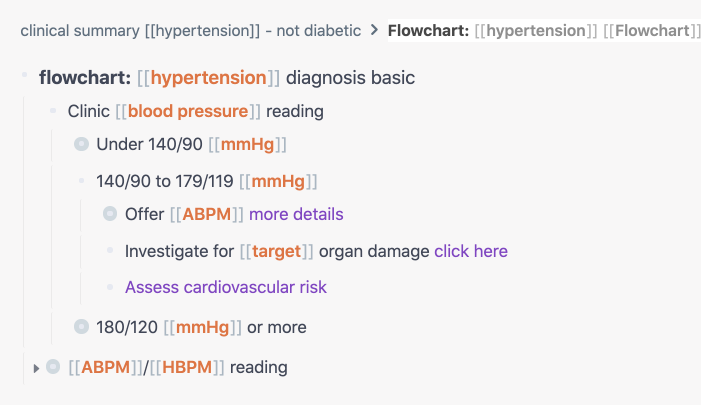
The advantage is that you only see what you need to see at any one time.
Writing for Roam or other networked medium
One thing we see when we start using the source material is that consistency is really important. In English we might say “[[[[liver]] function]]” or [[hepatic function]] and we might want a search to collect either version so it’s best to stick to one version.
Similarly, age is a big factor in disease. If we want to search for this topic in Roam, some standardised words or phrases might be useful to catch everything.
In addition, a word or short collection of words might have more than one possible searchable element. For example [[alo[[gliptin]]]] might be more effective than [[alogliptin]] to be able to find both the individual drug and the class “gliptins”. Or for chronic kidney disease, we might want to search for ‘kidney’, ‘kidney disease’ or ‘chronic kidney disease’.
When we go through a body of information like this, it seems that almost everything is linkable, which may create a readability problem for non-Roam users. On the other hand, it does show the utility of linking for this sort of knowledge. As I go through it linking words up, I feel like I’m sewing the information together, and making it tighter and more useful.
We also need to be aware of the size of the information block. We generally need fast, clear answers, so short sentences devoid of niceties, the passive tense and complicated words are preferred. The NICE Clinical Knowledge Summaries are great in this respect.
Future work
When I get time, I’ll keep adding to the database. I find it really useful for both learning and immediate reference. I showed it to a colleague and realised immediately that for most pharmacists to be able to use it, it needs to be really intuitive. Unfortunately, most people have little enthusiasm for learning how to use an app.
Some increase in usability, particularly on mobile, might be achievable with CSS. One simple thing for beginners might be to have automatically collapsing tabs, so that structure gets reimposed when you move away from a page.
What I’ve done is not the final answer, but it has been an interesting exercise in what is possible when you change the way you interact with information. I hope it stimulates some ideas.
It is valuable to consider how much more effective clinical practice could be if information retrieval methods were as seamless as memory. How much better might it be if someone could look across fields easily, rather than just being an expert in a siloed area? How might that change fields like nursing and pharmacy that are taking on more clinical roles? How might it change the ability to get good quality information in remote areas with limited access to medical staff or training?
I believe that the use of Roam can help to enable clinical knowledge to become much more effective and usable, and much easier to retrieve.